I have never really done any work on RTDs. I have an entire chapter on Casualties (Chapter 15) in War by Numbers, but nothing really on RTDS.
Anyhow, more than one person has asked me about this, so let me outline what I/we know:
1). The rule of thumb Trevor Dupuy developed on RTDs was in his “Handbook on Ground Forces Attrition in Modern Warfare,” September 1986, page 90. It says:
“Finally, there is a general rule of thumb for estimating returns to duty from casualties. For each 100 personnel casualties (battle casualty, disease, or injury) 75 will be returned to duty at the end of 20 days at a rate of five per day between the 6th and 20th days after admission, and 25 will never be returned to duty as a result of death, evacuation to the Zone of the Interior, or discharge. This will vary widely from situation to situation, depending in large part upon the theater evacuation policy.”
2). A report done by several people, including Ron Bellamy, who I have worked with, provides the following table:
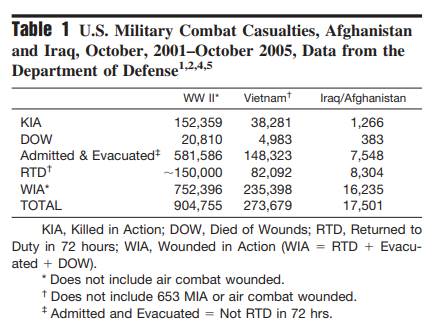
This chart is from this report: ADA480496.pdf (dtic.mil). I am indebted to Alex Roslin for this research.
Note that RTDs here is those that are returned within 72 hours. So, 752,396 WIA in WWII. Of those, 20% are RTD within 72 hours (and 2.8% are DOW). For Vietnam 235,398 WIA. Of those, 35% are RTD within 72 hours (and 2.1% are DOW). Note that these RTDs within 72 hours are probably all casualties “carded for record only.”
Note that the wounded-to-killed ratio for the WWII data is 4.94-to-1 or 4.22-to-1 if DOW is counted as KIA vice WIA and 3.36-to-1 if DOW is counted as KIA and RTD is not counted as WIA. The wounded-to-killed ratio for Vietnam data is 6.15-to-1 or 5.33-to-1 if DOW is counted as KIA vice WIA or 3.43-to-1 is RTD is not counted.
For the Iraq/Afghanistan data there are 16,235 WIA. Of those, 51% were RTD within 72 hours (and 2.4% are DOW).The wounded-to-killed ratio is 12.82-to-1 or 9.61-to-1 if DOW is counted at KIA vice WIA and 4.58-to-1 is RTD is not counted.
Now, I suspect some of the figures are skewed by how casualties are counted. In World War I and II, you were counted as wounded if you spent the night in a hospital. In Vietnam at one point the U.S. Army counted 96,900 wounded and maybe 104,000 carded-for-record only, meaning over 100,000 soldiers were not counted as wounded, but were allowed to receive the Purple Heart (my father got one that way). I may need to do a blog post about “carded for record” or WIANE (wounded-in-action, not evacuated).
See our report: “C-1 Combat Mortality: Why is Marine Combat Mortality Less than That of the Army (JCS) (March 1998),” page 19. This was done as a joint project with Ron Bellamy.
3). Now, where the “rule of thumb” that Trevor Dupuy came from is not known. In an attempt to find them, I pulled up three of the old HERO reports 1) 14. Historical Analysis of Wartime Replacement Requirements (26 July 1966), 2) 48. German and Soviet Replacement Systems in World War II (July 1975), and 3) 86. Analytic Survey of Personnel Replacement Systems in Modern War (Apil 1981).
In the second report, page 24 they do have a table “Table 3. German Replacement Army Strength, NCOs and Men, 1 September 1944” which has a total of 2,137,973 with “convalescents” making up 178.456 of that replacement army strength (8%). On 4 December 1944 (page 45) they show for November 1944 342,000 replacements of which 40,000 are convalescents (12%). And then on page 54 there are four tables, three which show convalescents. The most interesting is “Table 20: Losses and Arrivals, German Field Army. From July 1943 to March 1944.” It shows arrivals by month to the Eastern Front as 930,000, of which 421,000 are convalescents, 478,500 are replacements and 30,500 are FTDs (recruits sent to Feild Training Divisions). For “Other Fronts,” the numbers are much smaller: 24,000 convalescents and 50,000 replacements. What is interesting, but not surprising, is that the number of convalescents increase over time. From July through October 1943 it is 34,000 to 46,000 convalescents for each month, by February and March 1944 it is 60,000 convalescents a month.
For the Russians (page 90), the Germans estimated that 200,000 Russian convalescents were returned monthly to combat as replacements. The Germans estimated (page 91) that in 1942 ten Soviets armies received 764,000 replacements. Of them, new conscripts formed 56.5% of the total, 22.5% were convalescents, 10% were from labor battalions, 9.5% had been non-combat troops, and 1.5% had formerly had occupational deferments. Over 44,000, about 6%, were former convicts, released from prions and concentration camps.
For 1 January-31 August 1943 for sixteen Soviet armies the Germans estimated that 89% of the replacements were new conscripts, 9% were convalescents, and 2% were former non-combat and survivors of units destroyed. Also of interest is that the Germans estimated that 28% had training of less than 10 days, 49.6% had training of up to one month, and 22.4% had training of over one month. I will avoid the temptation to equate this with the current war in Ukraine.
A third report indicates that in June 1943, 34,384 Soviet replacements reached units (probably the Bryansk Army Group) facing the German Ninth Army as follows: 82% were new conscripts, 7% were convalescents, 11% were former non-combat. Their training was reported as 26% less than 10 days, 49% up to one month, and 11% were former non-combat.
Now, none of this actually answers my questions on RTD rates, but I still found it pretty damn interesting.
Finally, there is the report “Analytic Survey of Personnel Replacement Systems in Modern War.” This last report was primarily written by C. Curtiss Johnson (in case he is reading this blog).
It provides a few snippets of useful data. For example (page 48), it states for the 6695 and 6706 Conditional Companies (U.S. Army, Italy) that between 1 July 1944 and 10 June 1945 the two companies process approximately 12,400 patients, of whom nearly 10,400 were rehabilitated sufficiently to return to unit. This is 84% returned-to-duty.
In the case of the Vietnam War, the 90th Replacement battalion from the quarter ending 31 Jan 1969 through 31 October, processed 172,585 replacements and 175,346 returnees. Not sure this tells us much.
But this does… to quote (starting from page C-2):
Table 20, based on data compile by the Office of the Surgeon, MTOUSA, in December 1944, shows… the sample included 71,378 patients, 29,727 of whom had been injured and 41,651 of whom were battle casualties. Of the injured patients, 26,174 or 88.05% were returned to duty after hospitalization, 799 or 2,69% died, and 2,754 or 9.26% were evacuated to ZI hospitals. Of battle casualty patients (WIA), 29,860 or 71.69% were returned to duty, 1,130 or 2.71% died, and 10,661 or 25.60% were evacuate to ZI hospitals.
Experience during 1943-1944 showed that 86.69% of injury patients who were returned to duty became General Assignment personnel, and the remainder (13.31%) became Limited Assignment. The same figures for battle casualty patients were 83.89% General Assignment personnel and 16.11% Limited Assignment personnel.
…The General Board, ETO,… finding may be expressed in tabular form as follows:
Percentage of Returns Correlated to Theater Evacuation Policy
Days after Admission Battle Casualties (2,090) Non-Battle Cas. (100,000)
60 50.7 90.6
90 59.5 93.0
120 64.8 93.4
Of the total returned to duty, 28.6% of the battle casualties and 5.3% of the non-battle casualties were estimated to be Limited Assignment personnel. While no comparison can be made between the injuries surveyed by the Office of the Surgeon, MTOUSA, and the non-battle casualties surveyed by the General Board, ETO, the data for battle casualties in the two reports can be compared. This comparison shows that the MTO return rate (71.69%) much exceeded the greatest rate reported for the ETO (64.8%) and that the percentage of returned who became Limited Duty personnel was greater for the ETO (28.6%) than for the MTO (16.11%). The probable explanation for the disparity in these rates was the size of the populations surveyed: the ETO battle casualty sample was 2,090; the MTO sample was 41,651.
The Report of the Army’s postwar Replacement Board provides qualitative and quantitative assessments of the replacement value of hospitalized casualties. In Volume V, Annex 14, p. 1, Major General Russell B. Reynolds, who was ACS, G-1, SPA, stresses the replacement value of hospital returnees and comments:
When you sustain 10 battle casualties, you’ll bury 3, evacuate 2 to the US, find 4 suitable for return to duty in branch, and have to retrain, either in a training center, or on the job, 1. In the case of non-battle casualties, for each 10 you’ll evacuate about 4/10 of a man, bury 1/10 of a man, and find 8 2/4 suitable for return to duty in branch, and face a retraining job on 3/4 of a man.
These numbers may be expressed on a percent basis as follows: of surviving battle casualties, 28.6% will be evacuees and 71.4% will be returnees; of surviving non-battle casualties, 4.0% will be evacuees and 96% will be returnees. It is interesting to note that when these figures are compared to the same figures derived from MTO and ETO data, there is a remarkable degree of correlation.
The World War II data presented above may be compared to data developed from the statistical records of World War I by Colonel Albert G. Love of the US Army’s Medical Corps in 1931. Love found that in any typical group of AEF disease and non-battle injury (DNBI) patients, 3.70% would die, 7.52% would have to be evacuated (total lost 11.22%), and 88.78% would be returned to duty. For AEF battle casualty patients, excluding gas wounds, 8.12% would die, 29.58% would have to be evacuated (total lost 37.70%), and 61.88% would be returned to duty. The return rates for World War I DNBI casualties are very close to those of World War II, while World War I BC return rate is smaller than the smallest World War II BC return rate (ETO, General Board: 64.8%). The small World War I BC return rate undoubtedly reflects the less advanced medical treatment available in the earlier conflict (notice, for example, the greater percentage of BC patients dying in hospital).
Expressed in terms of AEF theater evacuation policies, Love’s data reveals the following:
Percentage of Returns Correlated to Theater Evacuation Policy
Percentage Returned to Duty
Days after Admission Battle Casualties DNBI
30 24.88 67.40
60 46.17 81.74
90 55.73 86.38
120 59.53 87.95
…The best, most recent set of data on the replacement value of hospitalized personnel is the data developed from the Korean conflict by Frank A. Reister… Reister’s Table 13, p. 14, shows the final disposition of 248,946 US Army patients from division units originating in Korea during July 1950 – July 1953. Of this number 72,961 were battle casualties (WIA) and 175,985 were non-battle casualties. The distribution of final disposition for battle casualties originating in division units was as follows: 2.2% (1,574) died of wounds, 87.9% (64,159) returned to duty, 8.5% (6,239) were separated for disability, and 1.4% (989) wee administrative separations. The distribution of final dispositions for division non-battle casualties was as follows: 0.3% (485) died, 98.6% (173,525) returned to duty, 0.9% (1,625) were separated for disability, and 0.2% (35) were administrative separations.
The return to duty figures developed by Reister may be compared to the same figures from Love’s compilation and the various World War II sets to indicate the relative increase in percentage of returns in the two admission categories since World War I and to underscore the value of hospital returnees as a source of replacements in future wars.
Bolding is mine. I suspect the bolded sentence was the basis of the Trevor Dupuy rule of thumb on RTDs.
In the end, there are over 140 old HERO, TNDA, DMSI and Trevor Dupuy reports. None that I have looked at clearly show where his “rule of thumb” on RTDs comes from, although it appears to have come from the last report referenced. I do have more old Dupuy files than I have time to look through them.
4) There is probably more material out there of value. If so, please post it to the comments in this blog.
5) Proselytizing note: I really did try a couple of years ago to get a probably study done on wounded-to-killed ratios and weapon lethality over time. Could never quite get the funding. Not sure why. See: Two proposals on Combat Casualties | Mystics & Statistics (dupuyinstitute.org)
If someone really wants the answers to these types of questions, then someone needs to start funding proper research.

Interestingly, the DoW/KIA ratio remains constant into the 60s, but does not carry over into the 2000s.
Looking at the Verlustwesen, from 39 to the end of 44, of the 5,240,000 WIA (Heer+Luft+Marine) there are 455,144 categorized as, “dismissed, unfit for service or readmission”.
Hi Chris, I understand it is not freely available: German and Soviet Replacement Systems in World War II (July 1975)?
It is available:
It is listed here: https://www.dupuyinstitute.org/tdipub1hero.htm
Ordering information is here: https://www.dupuyinstitute.org/order.htm
Comparing the number of KIA and wounWIA, I am confident that the Red Army did not take into account the losses of the lightly wounded. And the Germans counted the lightly wounded. in Krivosheev’s work on the losses of the Red Army for 1941-1945 there are more than 5 million KIA and less than 15 million WIA. less than 1 in 3! The Germans have a ratio of 1 to 4 for 1941-1944 on the East.