Sadly, there is plenty still to blog about with the coronavirus. The picture is changing enough from day-to-day that these updates are getting more frequent. At this point multiple countries have been shut down. They are now starting to shut down cities in the U.S. Yesterday Steven Mnuchin, our treasury secretary, was talking about possibly 20% unemployment. This thing is going to have a big impact and it is affecting everything (including national security issues and future defense spending). I will be blogging about this for a while.
China continues to report very few new cases. For the last eight days they have consistently reported 80.9K to 81K cases. So it is only growing by a few dozen cases a day. Friday it was 80,945, Saturday it was 80,976, and as of Sunday night it was 81,020 and this morning (Wed) it is 81,102. This is 157 new cases in the last four or five days or less than 40 cases a day. So, almost under control, but not quite. If one relaxes some of the restrictions for the sake of getting the economy working again, what happens?
Country……….Cases……Deaths……Rate
World Wide……204,255….8,243…..…4.04%
China.……………81,102….3,237…..…3.99%
Italy………………31,506….2,503…..….7.94%
Iran………….…..17,361…..1,135…..….6.54%
Spain……….…..13,910..……623………4.48%
Germany………..10,082………26…..….0.26%
S. Korea…….……8,413………84…..….1.00%
France…………….7,696……..148…..….1.92%
United States…….6,510…….114…..….1.83%
Switzerland………2,700……….27…..….1.00%
Netherlands.……..2,056.…..….58.….….2.15%
United Kingdom…1,961……….71………3.62%
Norway……………1,527..….……6………0.39%
Belgium….…….…1,486………14…..…..0.94%
Austria……………1,471..…….…3……….0.20%
Sweden…..………1,212…………8….…..0.66%
Denmark..………..1,091…………4…..….0.37%
Sixteen countries around the world with over a thousand cases. Below is a list of some of the rest. They are mostly European but countries from all over the world are joining the list. Not sure how much more extensive testing influences these figures.
Country……..…Cases……Deaths……Rate
Japan………………889..……….29.……..3.26%
Malaysia….…..……790…………2………0.25%
Canada……..……..598………….8….…..1.34%
Australia……………568..….….…6….…..1.06%
Czech Rep…………464……….…0….…..0%
Portugal.…..….……448……….…2……….0.45%
Qatar..……………….442..……..…0….…..0%
Israel…….…….……427…………..0….…..0%
Greece..….……..….387……….…5………1.29%
Brazil……………….350…..…..…2………0.57%
Finland….…………..336……….…0………0%
Singapore…..………313…………0………0%
Ireland……………..292……….…2.……..0.68%
Slovenia….………..275…..…..…1………0.36%
Estonia…..…………258…………0………0%
Bahrain………….…256…………1….…..0.39%
Pakistan………….…256…………0…..…..0%
Poland………….…..251…………5……….1.99%
Iceland………….…..250…..….…1….……0.40%
Romania……………246…………0……….0%
Chile..………………238………….2…..….0.84%
Indonesia….……….227………..19……….8.37%
Thailand.…..……….212…………1………0.47%
Luxembourg.….…..203…..…..…2………0.99%
Philippines…….…..202………..19….…..9.41%
Egypt………………196……….…6…..….3.06%
Hong Kong……..…181……….…4………2.21%
Saudi Arabia………171…………..0………0%
Iraq…..……………..164..…….…12…..….7.32%
India…….….………152………..…3.……..1.97%
Russia…….…….…147………..…0……….0%
Kuwait……….…….142..…………0…..…..0%
Lebanon……..….…133..…………3….……2.26%
San Marino…………119………….11….…..9.24%
Peru………….………117………..…4……….3.42%
South Africa…..……116………..…4……….3.45%
UAE……………..….113………..…0…..….0%
Ecuador.….…..……111………..…2……….1.80%
Taiwan…………..…100…..……….1…..…..1.00%
Turkey…………….….98…..……….1….……1.02%
Slovakia…………..….97………..…1….……1.03%
Mexico…….….………93………..…0….……0%
A few other entities of interest to this author that have less than 98 cases so far:
Vietnam….……….…68…………0……..…..0%
Azerbaijan..….………28……..…1………….3.57%
Palestine…..…………26?……….0………….0%
Afghanistan….………22……..…0………….0%
New Zealand…….….20……..…0…………0%
Ukraine…………..…..14.…….…2…….….14.29%
North Korea..…………0……..…0…….……0%
Syria……….…………..0………..0…….……0%
Diamond Princess……712……..7………….0.98%
Part of my concern is the spread of the disease across the Middle East and Central Asia. There are a number of countries in the region still at war, including Syria, Afghanistan and Iraq. How does one contain a virus in a country at war? Do they then serve as a vector for the rest of the countries in the region?
Data is from Johns Hopkins CSSE 3/18/20 as of 9:33.12 AM EST. It was updated thrice while I was writing this. It is here: Johns Hopkins CSSE
A few more observations:
- It does appear that at best the mortality rate is around 1% if: 1) there is good health care and 2) there is good reporting. That appears to be borne out by the reporting from South Korea and the more contained environment of the cruise ships.
- The S. Korean mortality rate is now at 1%. They have tested more than 240,000 of their people. This is about a good and complete reporting as we are going to see in the real world. It is getting harder to make the argument that the mortality rate is much less than 1%, even assuming a large number of cases were not reported.
- Most other countries with a reported rate of less than 1% I suspect have just recently gotten a number of new cases and these figures will be unfortunately changing over time (for example Germany).
- If mortality really is around 1% or less, then it appears there are already over 250,000 in cases Italy and over 100,000 cases in Iran.
- Now it could be that the natural mortality rate in Italy will be higher than what we are seeing for S. Korea. This will be explored in a future post.
- San Marino has a population of 33,562. With 119 cases, this makes it the “most infected” country in the world with 0.35% infected.
- The Holy See (Vatican City) is second with 1 case in around 1,000 people (0.10%)
- Italy with 60,317,546 people and 31,506 cases is third (0.052%)
- If they really have over 250,000 cases then we are looking at over 0.4%, a figure similar to San Marino (which makes sense).
- Iran is now fourth with population of 83,183,741 and 17,361 cases. This is 0.021% infected. If they have over 100,000 cases then this is 0.12% infected.
- South Korea with 51,709,098 people and 8,413 cases is now fifth (0.016%)
- I still suspect 44 U.S. passengers from the Diamond Princess are being double counted in CSSE database. They are now listed as a subset of the Diamond Princess button, but I suspect they are still being counted in the U.S. totals.
- Also, Hong Kong’s 181 cases are also counted under China. I just choose to separate out Hong Kong because there is a political protest movement of some significance going on there.
- Palestine was reported last Wednesday to have 26 cases. Now the CSSE database does not report on Palestine. Not sure where those 26 cases went to. Are they reported under Israel?
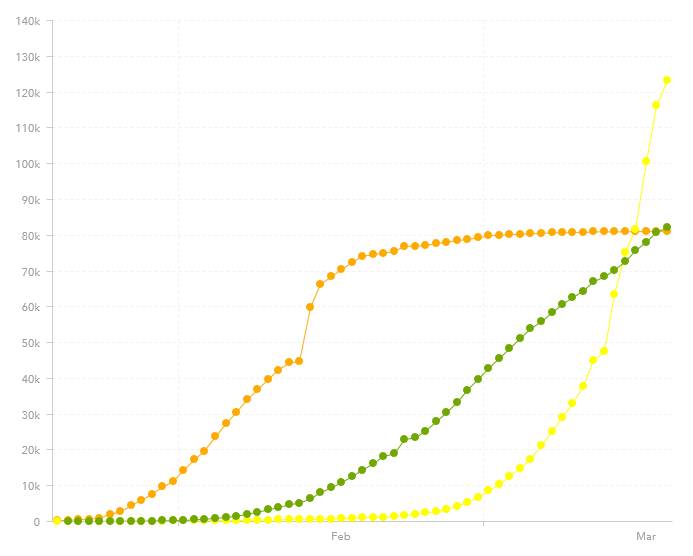
On the graph at the top of this post, the new top line is the number of coronavirus cases in “other locations” (meaning outside of mainland China). The original top line is the number of coronavirus cases in Mainland China (People’s Republic of China). The next line is the “Total Recovered” which is reported at 82,107 out of 204,255 cases (and 8,243 deaths). It has now just passed the Mainland China line.

“The S. Korean mortality rate is now at 1%. They have tested more than 240,000 of their people. This is about a good and complete reporting as we are going to see in the real world. It is getting harder to make the argument that the mortality rate is much less than 1%, even assuming a large number of cases were not reported.”
That is a not good interpretation of available data.
1) Maximum test capacity is more or less a constant in a country. Number of infected people not. Tests will hit a ceiling quite early. This leads to a increasing “mortality”.
2) Not only the number of tests is important, but also efficiency of testing, i.e. how many cases are identified with 100 tests.
While South Korea was very early testing at a quite high number, the test efficiency is low, they need 30 tests to identify one infected person. That did not matter at the beginning, but now gives a higher ratio deaths/tested cases.
In contrast, the Austrians and most likely the Germans test with a three times higher efficiency, i.e. they need less than 10 tests to identify one infected person. These countries will meet the saturation of the test infrastructure later.
The only hard data we have are the number of dead patients. Therefore, you should check ratio of identfied cases per dead patient and performed tests per dead patient. Then you can use the same (relative) time point for this analysis: the first dead patient in each country and use cases per 1 million citizens.
The ratio deaths/identified cases is only near the real mortality at the beginning of the pandemic in countries where testing started early in high numbers, therefore rates determine BEFORE saturation of the test capacity are relevant.